catastrophic antiphospholipid antibody syndrome
- related: Hematology
- tags: #literature #hemeonc
The catastrophic antiphospholipid antibody syndrome requires evidence of involvement of three or more organs, systems, and/or tissues that develops in 1 week or less with laboratory confirmation of antiphospholipid antibodies. Additionally, evidence of small vessel occlusion in at least one organ or tissue by histopathology is required for definitive diagnosis.
This patient has evidence of lung, kidney, and hematologic involvement with evidence of bleeding, as well as arterial and venous thrombosis all occurring within days. Additionally, she is anti-β2 glycoprotein I antibody positive and has histopathological evidence of vessel occlusion. The histopathology slide images from renal biopsy demonstrate a thrombosed small artery surrounded by renal tubules (Figure 2) and an arteriole at the base of a glomerulus with thrombosed glomerular capillaries (Figure 3).
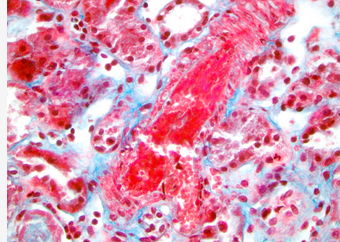
Thrombotic microangiopathy (400× magnification). Histology image courtesy of Dr. Bruce Jones of Henry Ford Hospital, Detroit, MI, USA.
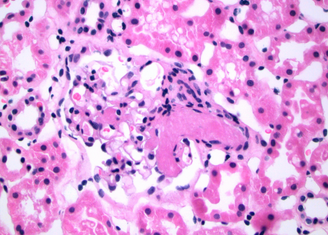
An arteriole at the base of a glomerulus with a few thrombosed glomerular capillaries is seen (400× magnification). Surrounding tissues are renal tubules.
The catastrophic antiphospholipid syndrome is reported to be seen in <1% of patients with antiphospholipid antibodies. Anticoagulation (in the absence of frank bleeding), corticosteroids, and plasma exchange are mainstays of treatment (choice C is correct).
There is no consensus on absolute criteria needed for the diagnosis of disseminated intravascular coagulation (DIC). Common laboratory criteria include thrombocytopenia, prolonged prothrombin time and activated partial thromboplastin time, low plasma fibrinogen, and elevated plasma D-dimer. DIC can present after trauma, with sepsis, or as a result of malignancy. It often manifests as bleeding (oozing from sites of trauma, catheters, or drains). Microangiopathic changes on peripheral blood smear may also be seen. Several diagnostic criteria for DIC have been proposed with prothrombin time, platelet count, fibrinogen, fibrinogen degradation products, and D-dimer being used for scoring. This patient only exhibits bleeding and thrombocytopenia, which may be insufficient to establish the diagnosis of DIC based on these scoring systems (choice A is incorrect).
Thrombocytopenic thrombotic purpura (TTP) is characterized by thrombocytopenia accompanied by microangiopathic hemolytic anemia. Laboratory testing in TTP reveals elevated lactate dehydrogenase, low haptoglobin, and schistocytes >2/high-power field. The Coombs test is negative in TTP, as the hemolytic anemia is not from an immune process, but from mechanical shear stress. An ADAMTS13 level <10 is characteristic of TTP but is not always seen (choice B is incorrect).
1Microscopic polyangiitis is the most common etiology of pulmonary-renal syndromes. Patients present with fever and with laboratory testing that reveals elevated sedimentation rate, elevated C-reactive protein, elevated creatinine, and anemia. Serology is usually positive for myeloperoxidase perinuclear antineutrophil cytoplasmic antibodies (choice D is incorrect).23145
A 25-year-old woman with no significant past medical history presents with nausea, vomiting, and abdominal pain for the past 2 days. She does not drink alcohol. She has two bouts of hematemesis in the ED. A urine pregnancy test is negative. Her hemoglobin is 7.1 g/dL (71 g/L). Upper endoscopy is performed, which reveals antral gastric ulcers. She is started on proton pump inhibitor therapy. The following day, she develops a temperature of 39.3°C, respirations of 24/min, and SpO2 of 85% on room air. She is intubated and mechanically ventilated. Shortly after stabilization on the ventilator, you notice bloody secretions in the endotracheal tube. The chest radiograph is shown. You perform bronchoscopy with BAL, which reveals progressively worsening bloody effluent with serial aliquots. Her creatinine is 4.28 mg/dL (378.35 µmol/L), BUN is 86 mg/dL (30.70 mmol/L), and platelet count is 80 × 103/μL (80 × 109/L). Her total bilirubin is 0.8 mg/dL (13.68 µmol/L), and direct bilirubin is 0.2 mg/dL (3.42 µmol/L). There is large blood on urinalysis, and 50 to 80 RBCs per high-power field on urine microscopy. Renal biopsy is performed. A peripheral blood smear reveals dimorphic RBCs, thrombocytopenia, and leukopenia with toxic changes in polymorphic neutrophils. No schistocytes are seen, and ADAMTS13 level is normal. Fibrinogen is 200 mg/dL (5.88 g/L), prothrombin time is 17.8 s, and partial thromboplastin time is 55 s. C3 complement is 9 mg/dL (0.09 g/L), and C4 complement is 3 mg/dL (0.03 g/L). Antinuclear antibody is strongly positive, DNA antibody is strongly positive with 1:160 titer, and rheumatoid factor is normal. Antineutrophil cytoplasmic antibodies are normal. Ribonuclear antibody is positive, anti-Sjögren’s-syndrome-related antigen A Ro/anti-Sjögren’s-syndrome-related antigen B La ab are both positive. Sedimentation rate is 7 mm/h (normal). Anti-β2 glycoprotein I antibody is positive. Three days later she is diagnosed with a deep vein thrombosis of her right lower extremity. What is the most likely diagnosis?
Links to this note
Footnotes
-
Espinosa G, Rodríguez-Pintó I, Cervera R. Catastrophic antiphospholipid syndrome: an update. Panminerva Med. 2017;59(3):254-268. PubMed ↩ ↩2
-
Carmi O, Berla M, Shoenfeld Y, et al. Diagnosis and management of catastrophic antiphospholipid syndrome. Expert Rev Hematol. 2017;10(4):365-374. PubMed ↩
-
Taylor FB Jr, Toh CH, Hoots WK, et al; Scientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86(5):1327-1330. PubMed ↩
-
Wada H, Matsumoto T, Yamashita Y. Diagnosis and treatment of disseminated intravascular coagulation (DIC) according to four DIC guidelines. J Intensive Care. 2014;2(1):15. PubMed ↩