constrictive pericarditis vs restrictive cardiomyopathy
- related: Cardiology and Hemodynamics
- tags: #literature #cardiology
Distinction between constrictive pericarditis and restrictive cardiomyopathy can be important because constriction is a potentially curable cause of heart failure and options for restrictive cardiomyopathy are limited.
In patients such as this one, who have had mediastinal radiation, both are possibilities. A Kussmaul’s sign is a rise in jugular venous pressure with inspiration (Kussmaul sign in pericarditis). Ordinarily jugular venous and right atrial pressure decrease as intrathoracic pressure decreases, augmenting venous return to the right heart, but in constrictive pericarditis, the heart has a fixed volume due to encasement by the pericardium, and negative intrathoracic pressure with inspiration is not transmitted to the heart. Because the pulmonary veins are intrathoracic but not intracardiac, negative inspiratory pressure decreases left-sided filling and allows for increased right ventricular (RV) volume at the expense of left ventricular (LV) volume. In constriction, this increased right-sided volume with inspiration causes an increase in right atrial pressure. The Kussmaul’s sign was originally identified in a patient with constrictive pericarditis, but occurs in only one-third of cases, and can be seen in other conditions that cause right-sided failure, including restrictive cardiomyopathy if the right ventricle is involved. Significant pericardial constriction limits the total volume of blood that can be accommodated by the heart and increases the venous pressure required for right-sided filling.
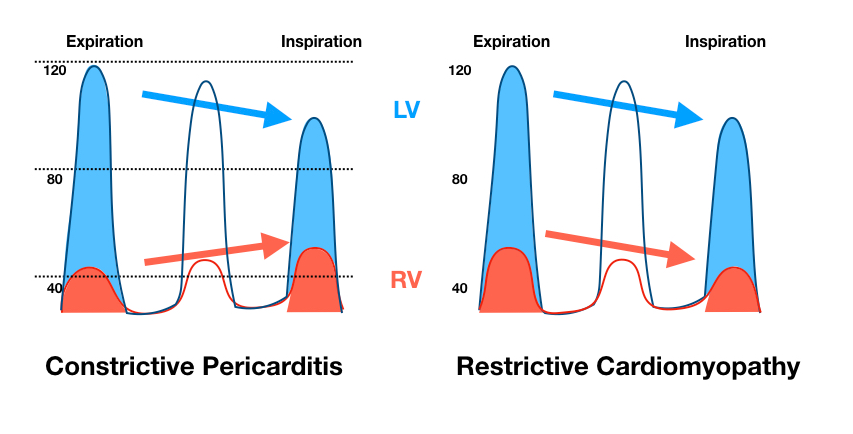
Early right-sided diastolic filling is increased due to high right atrial pressure, producing a rapid y (diastolic) descent on the jugular venous waveform, but pressure rises rapidly and then stops as the heart reaches the limits of pericardial constraint, producing a classic “square-root” sign. A characteristic feature of constrictive pericarditis is ventricular interaction with respiration (increased volume of one ventricle at the expense of the other) for the reasons described. Because of this interaction, there is disjunction between RV and LV pressures with respiration, such that one goes up as the other goes down. See Figure 1 (choice C is correct).
This is best demonstrated by simultaneous measurement of RV and LV pressures in the cardiac catheterization laboratory and has been shown to be the most sensitive and specific sign of pericardial constriction. Right atrial pressure is increased in both constriction and restriction (choice A is incorrect). Pericardial constriction might be expected to produce RV diastolic dysfunction with an increased ratio of RV end-diastolic to RV end-systolic pressure, and LV end-diastolic pressure minus RV end-diastolic pressure might be expected to be higher in restrictive cardiomyopathy, but neither of these signs has been shown to have either good sensitivity or specificity in distinguishing between the two (choices B and D are incorrect).123
A 35-year-old woman presents with shortness of breath. She had been having dyspnea on exertion and leg swelling for several months but now is having abdominal discomfort and is dyspneic at rest. Her history is significant for Hodgkin’s disease treated with chemotherapy and mediastinal radiation at age 27. BP is 86/68 mm Hg, heart rate is 105/min, respiratory rate is 26/min, and temperature 37.1°C. She has jugular venous distension that increases with inspiration. Her lungs are clear, and her cardiac exam is normal. She has hepatomegaly and severe bilateral edema. Her ECG is normal except for tachycardia. Point-of-care ultrasound reveals normal cardiac function without a pericardial effusion, no B lines suggestive of pulmonary congestion, and ascites. Which of the following hemodynamic findings is most useful to distinguish constrictive pericarditis from restrictive cardiomyopathy in this patient?