cyanide toxicity causes, symptoms, labs
- related: cyanide toxicity
- tags: #literature #icu
When a patient presents with altered mental status and unexplained metabolic acidosis, cyanide poisoning should be considered.
Cyanide avidly binds the ferric ion (Fe3+) of cytochrome oxidase a3, inhibiting its enzymatic activity in the mitochondrial cytochrome complex and uncoupling oxidative phosphorylation.
The result is anaerobic metabolism to produce adenosine triphosphate and the formation of lactic acid, causing metabolic acidosis. Serum bicarbonate levels fall in an attempt to buffer excess acid. Metabolic acidosis also triggers central and peripheral chemoreceptors, increasing alveolar ventilation and then presenting as tachypnea. This leads to a fall in arterial PCO2 (PaCO2).
Cyanide poisoning may result from a broad range of exposures, but the most common is fire. Cyanide can be released during the combustion of products containing both carbon and nitrogen, including many household products such as wool, silk, polyurethane (upholstery), plastics (polyacrylonitriles), and synthetic rubber. The marked lactic acidosis in this patient, despite normal oxygenation and low carboxyhemoglobin levels, should prompt consideration of cyanide poisoning from the combustion of household products.
Another cause includes nitroprusside use in hypertensive emergency. Nitroprusside is a potent vasodilator that works on both arterial and venous circulation and is used for hypertensive emergency management. It has rapid onset and offset of action. The most important side effect is cyanide accumulation and toxicity.
Symptoms include headache, confusion, loss of consciousness, and seizures. Patients are usually tachycardic and hypertensive initially but may develop bradycardia and hypotension and arrhythmias later. Tachypnea is usually present, and mild pulmonary edema may be seen, with cyanosis fairly common.
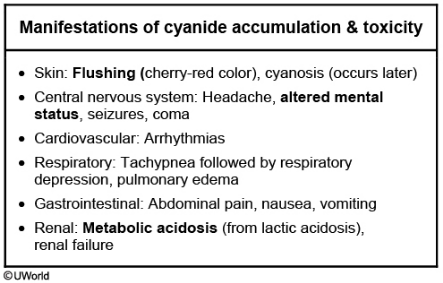
Cyanide poisoning impairs the use of oxygen by tissues, resulting in an abnormally high venous SpO2 (ie, venous hyperoxia). This results in a narrowed venous-arterial PO2 gradient, like that seen in this patient. The high venous SpO2 results in a bright red appearance to venous blood, which rarely causes the skin to flush cherry red. Renal failure and hepatic necrosis can occur, and rhabdomyolysis is also frequently seen.12345
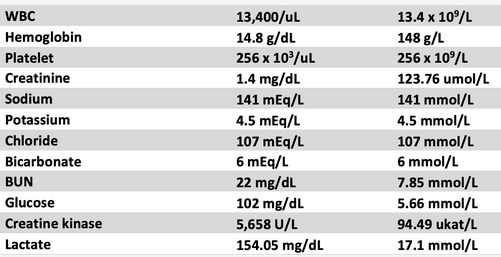
A 28-year-old man is admitted to the ICU after being found unconscious in his smoke-filled apartment where his couch was on fire. He was brought to the hospital on 100% oxygen via face mask and awoke en route. He is awake but mildly confused and does not know what happened. SpO2 is 100% on a 100% nonrebreather mask. Vitals include a respiratory rate of 30/min, heart rate of 126/min, and BP of 165/92 mm Hg. His skin has a cherry red color. Labs include the following (Figure 1) (the normal values for creatine kinase are 40 to 150 U/L [0.67 µkat/L to 2.5 µkat/L]).
Arterial blood gas demonstrates a pH of 7.08, PCO2 of 21 mm Hg, and PO2 of 228 mm Hg, with CO-oximetry demonstrating 0.3% methemoglobin and 5.2% carboxyhemoglobin. Central venous SpO2 is also 100%, with a mixed venous oxygen tension of 199 mm Hg.
Which of the following is the best next step in the treatment of this patient?
A 38-year-old African American man comes to the emergency department after experiencing severe back pain for the past 2 days. He has a history of hypertension for the last 5 years. His current medications include hydrochlorothiazide, amlodipine, and valsartan. The patient has a 15-pack-year history and drinks 4-5 bottles of beer daily. His temperature is 36.7 C (98 F), blood pressure is 230/112 mm Hg, and pulse is 84/min. Funduscopic examination shows arteriolar wall thickening and occasional cotton-wool spots. The rest of the examination is within normal limits. Initial laboratory studies show serum blood urea nitrogen of 28 mg/dL, potassium of 5.1 mEq/L, and serum creatinine of 2.3 mg/dL. Transesophageal echocardiogram is consistent with dissection in the descending aorta. The patient is admitted to the coronary care unit and started on intravenous labetalol and nitroprusside infusion. The next morning, the nurse finds him confused and agitated. He then has a generalized tonic-clonic seizure. His temperature is 36.7 C (98 F), blood pressure is 176/99 mm Hg, and pulse is 102/min. Physical examination remains otherwise unchanged.
Which of the following is the most likely diagnosis?
Links to this note
-
- cyanide toxicity: cyanide toxicity causes, symptoms, labs
Footnotes
-
Baud FJ, Barriot P, Toffis V, et al. Elevated blood cyanide concentrations in victims of smoke inhalation. N Engl J Med. 1991;325(25):1761-1766. PubMed ↩
-
Mokhlesi B, Leikin JB, Murray P, et al. Adult toxicology in critical care: Part II: specific poisonings. Chest. 2003;123(3):897-922. PubMed ↩
-
Parker-Cote JL, Rizer J, Vakkalanka JP, et al. Challenges in the diagnosis of acute cyanide poisoning. Clin Toxicol (Phila). 2018;56(7):609-617. PubMed ↩
-
Shepherd G, Velez LI. Role of hydroxocobalamin in acute cyanide poisoning. Ann Pharmacother. 2008;42(5):661-669. PubMed ↩