diagnosis of ABPA includes eosinophil count, antibody level, and CT image findings
- related: Allergic bronchopulmonary aspergillosis ABPA, aspergillosis
- tags: #permanent
- source: uptodate, Fundamentals of High Resolution Lung CT
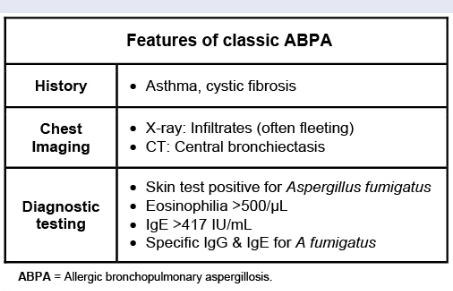
Patients are usually predisposed with asthma or CF. COPD patients are also at risk for ABPA. Diagnosis includes CT image findings (unilateral, asymmetrical, central bronchiectasis with mucous impaction) and labs:
- Total IgE > 1000
- aspergillus fumigatus IgE elevated
- eosinophil count > 500
- patients: underlying asthma, CF
- pathogenesis: sensitization to aspergillus, intense IgE and IgG mediated immune response
- sx: recurrent exacerbations. Sx of pneumonia in asthma patient unresponsive to treatment
- dx:
- elevated Aspergillus-specific IgE
- elevated (eg, >417 IU/mL) total IgE
- positive Aspergillus-specific IgG
- eosinophilia
- positive skin test reactivity for Aspergillus.
- Consequently, the initial evaluation for ABPA should include either skin testing for Aspergillus or analysis of total and specific IgE concentrations.
- cxr: upper lobe opacities, atelectasis due to mucus plugging, and signs of bronchiectasis such as bronchial wall thickening.
- rx: steroids as this is hypersensitivity reaction
- sometimes supplemented by antifungal with azole
Links to this note
- cystic fibrosis
- CF patients are at increased risks for ABPA: diagnosis of ABPA includes eosinophil count, antibody level, and CT image findings.
- Allergic bronchopulmonary aspergillosis ABPA
- aspergillosis
- pulmonary eosinophilia differential diagnosis