epidural bleed management
- related: Neurology
- tags: #literature #neuro
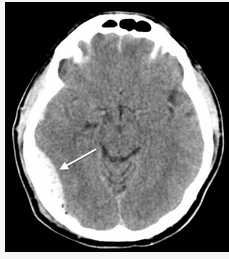
This is a typical case of an epidural hematoma. Unlike the more common subdural hematoma, which is usually due to slow venous bleeding, epidural hematomas are typically due to disruption of the middle meningeal artery, which leads to blood accumulation at arterial pressure. The classic syndrome associated with epidural hematoma includes initial loss of consciousness followed by a short lucid period when patients are often confused and, finally, lose consciousness as the blood exerts enough pressure on the brain to compress brainstem structures.
The blood collection shows the classic biconvex hematoma (Figure 2). Although this syndrome is commonly taught in medical school using pediatric cases as the example, it can be overlooked in older patients and represents a missed opportunity for timely treatment.
After the diagnosis of epidural hematoma, treatment is straightforward but differs from treatment of other intracranial hemorrhages. Unlike intraparenchymal hemorrhage and subdural hematomas, BP control is thought to be detrimental, as it is a compensatory mechanism to overcome the pressure development in the calvarium and because lowering arterial pressure is unlikely to prevent further bleeding. In addition, because of the rapidity of the development of pressure and the high risk of early death, initiation of measures to control intracranial pressure are seen as unproductive and could possibly delay definitive treatment. The only treatment definitively shown to reduce death is the immediate evacuation of the hematoma. All efforts should be focused on that goal alone. In many cases, hyperventilation is initiated as a bridge to the patient getting to surgery. Care must be taken to prevent severe alkalosis (PCO2 <20 mm Hg), as this can lead to brain ischemia. Interestingly, the mortality of epidural hematomas has decreased in the era of organized emergency care and trauma resuscitation. Historical mortality rates of up to 30% have decreased in a recent review to 7%. Many of the traditional risk factors for poor outcome such as hypovolemic shock and prolonged time to surgery are no longer associated with increased mortality (largely because they occur so infrequently). Two risk factors that persist for poor outcome are the presence of alcohol intoxication and extracranial trauma.123
A 37-year-old man with a history of alcohol use disorder is in an altercation in a bar and falls down a flight of stairs. He initially gets up from the base of the stairs and sits down. Approximately 6 min after the initial fall, he becomes unresponsive. The emergency medical service is called, and he is transferred intubated to the ICU. After emergent CT scanning (Figure 1), the patient is found to be hypertensive, with a BP of 180/72 mm Hg, tachycardic to 115/min, and breathing spontaneously with pressure support ventilation. On neurological exam, he is poorly responsive to painful stimulus, with flexor posturing on the right side and localization on the left side. The next appropriate treatment is which of the following?
Links to this note
Footnotes
-
Gutowski P, Meier U, Rohde V, et al. Clinical outcome of epidural hematoma treated surgically in the era of modern resuscitation and trauma care. World Neurosurg. 2018;118:e166-e174. PubMed ↩
-
Rivas JJ, Lobato RD, Sarabia R, et al. Extradural hematoma: analysis of factors influencing the courses of 161 patients. Neurosurgery. 1988;23(1):44-51. PubMed ↩