evacuate blood in IVH
- related: Neurology
- tags: #literature #neuro
Intracerebral hemorrhage with predominant intraventricular hemorrhage (IVH) has been a challenging disease because the expectations of providers and the real outcomes are often discordant. Because IVH affects a fluid-filled space as opposed to the parenchyma of the brain, the expectation is that the patient should recover without significant sequelae. This is clearly not the case; a study using the control populations of other studies with EVD placement and BP control showed mortality rates of 56%. In practice, the reasons for the increased mortality include poor consciousness due to the intracerebral hemorrhage component, recurrent complications from hydrocephalus in ventricular fluid diversion, and complications of ICU care. Studies using fibrinolytics to remove blood have shown improvement in mortality.
Until these studies, no strategy for management of external ventricular drainage had been shown to improve mortality after IVH.
The most recent development in the treatment of IVH has been the administration of tissue plasminogen activator (tPA) into the cerebrospinal fluid to aid in the dissolution of blood clots, allowing for drainage of unclotted blood from the ventricles. This technique was first pioneered using streptokinase; now tPA is favored due to the ease of use and suspected improved safety. Interestingly, multiple studies have shown improved mortality with the use of tPA. Skeptics worry that the improved mortality leaves more patients with a poor neurological outcome. The most recent randomized trial, CLEAR III, shows that in the group of patients with >20 mL of intraventricular blood in whom 85% of the blood can be cleared from the ventricular space, functional outcome is also improved. For this reason, the patient described is in a group that would benefit by improved mortality but also improved outcome.1234
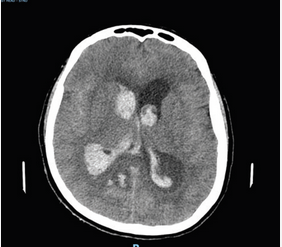
A 60-year-old woman presents with the acute onset of headache. The initial CT scan is shown (Figure 1). An external ventricular drain (EVD) is placed. Which intervention has been shown to decrease the risk of mortality?
Links to this note
Footnotes
-
Abdelmalik PA, Ziai WC. Spontaneous intraventricular hemorrhage: when should intraventricular tPA be considered? Semin Respir Crit Care Med. 2017;38(6):745-759. PubMed ↩
-
Wang D, Liu J, Norton C, et al. Local fibrinolytic therapy for intraventricular hemorrhage: a meta-analysis of randomized controlled trials. World Neurosurg. 2017;107:1016.e1-1024.e1. PubMed ↩
-
Ziai WC, Tuhrim S, Lane K, et al; CLEAR III Investigators. A multicenter, randomized, double-blinded, placebo-controlled phase III study of Clot Lysis Evaluation of Accelerated Resolution of Intraventricular Hemorrhage (CLEAR III). Int J Stroke. 2014;9(4):536-542. PubMed ↩