IMT inflammatory myofibroblastic tumor
- related: lung mass and cancer
- tags: #literature #pulmonology
- disease: 1.inflammatory myofibroblastic tumor IMT
- patient population and frequency: 2.50% of benign lung lesions in children
- gene: 2.anaplastic lymphoma kinase translocation
- CT: 2.well circumscribed, surrounding GGO, isolated lesion
- histology: 2.spindle cell
The histopathology shows a fibrolymphoplasmacytic infiltrate most consistent with an inflammatory myofibroblastic tumor (IMT). IMTs have anaplastic lymphoma kinase translocations approximately 50% of the time (choice C is correct).
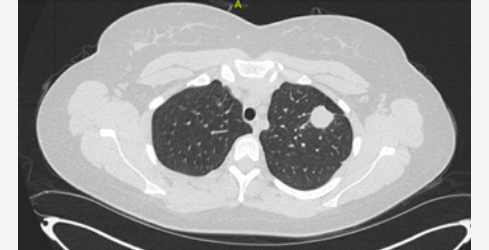
IMTs are rare mesenchymal neoplasms in adults, while they may represent up to 50% of benign lung lesions in children. They can occur in many sites throughout the body. When involving the lungs, they may be asymptomatic or present with nonspecific respiratory or systemic symptoms. They are most commonly seen in the lower lobes and in the lung periphery. They are often well circumscribed on imaging and can have surrounding ground-glass change. IMTs typically have an indolent course, with surgical resection recommended for cure. Tumor recurrence, malignant transformation, and metastatic disease can occur. Histologically, spindle cell proliferation and inflammatory infiltrate, with lymphocytes and plasma cells, is seen (Figure 7). IMTs have been associated with infections and systemic inflammatory conditions, at times listed under the broader label of inflammatory pseudotumors. Lung involvement from IgG4-related disease has an overlapping appearance. Approximately 50% of IMTs have a translocation of the anaplastic lymphoma kinase gene, providing a target for therapy if the disease is unresectable.1
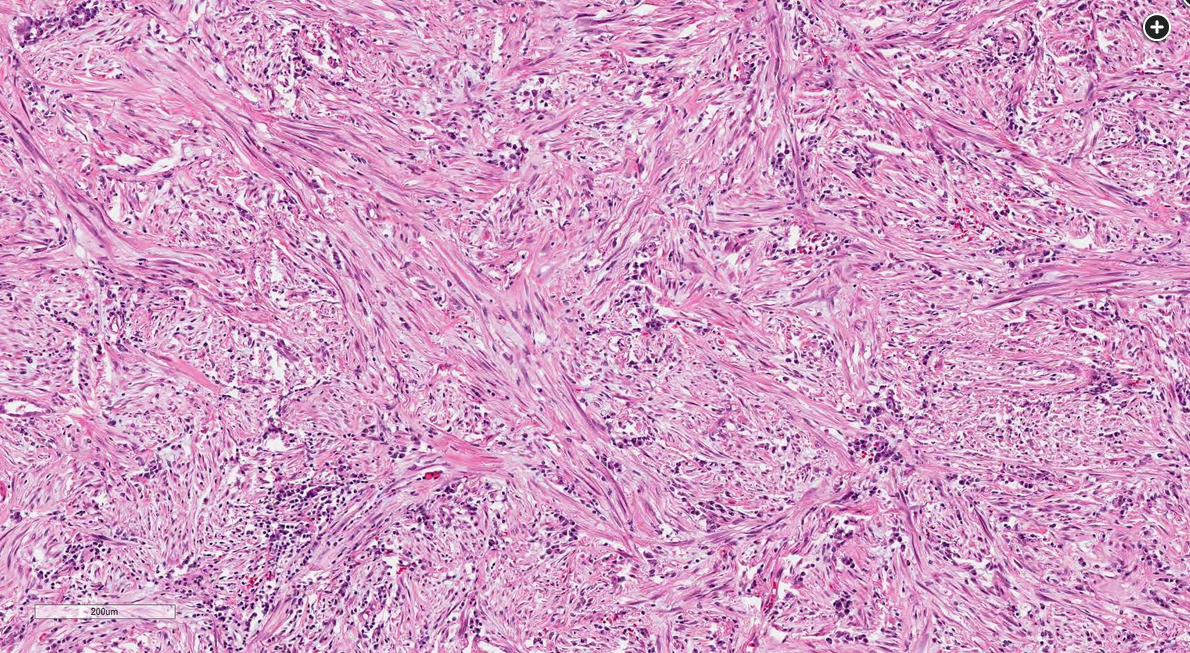 Spindle cell proliferation and inflammatory infiltrate, with lymphocytes and plasma cells compatible with an inflammatory myofibroblastic tumor. H&E stain, ×40 magnification.
Spindle cell proliferation and inflammatory infiltrate, with lymphocytes and plasma cells compatible with an inflammatory myofibroblastic tumor. H&E stain, ×40 magnification.