pediatric pulmonary tumors
- related: lung mass and cancer
- tags: #literature #pulmonology
- pulmonary carcinoid tumors are slow growing neuroendocrine tumor
- hamartomas are slow growing tumors with fat and cartilage
- IMT inflammatory myofibroblastic tumor
Most solid organ tumors can metastasize to the lung. In the age range of the patient in this question (20 year old), a primary carcinoid tumor of the lung, sarcoma, germ cell tumor, or extranodal lymphoma are more likely than a primary lung cancer.
There are many benign etiologies of lung nodules. Fungal and mycobacterial infections can present as a single nodule or multiple lung nodules with or without adenopathy. Bacterial abscesses and parasitic infections may also present as lung nodules. Benign tumors, most commonly hamartomas, bronchogenic cysts, and vascular lesions (such as arteriovenous malformations) can be considered. Inflammatory nodules such as rheumatoid nodules, those related to sarcoidosis, inflammatory bowel disease, and granulomatosis with polyangiitis, as well as benign lesions that do not fit into another category (eg, amyloid nodule, rounded atelectasis, intrapulmonary lymph nodes) round out the list.
The clinical features of the patient (demographics, smoking history, comorbidities, active symptoms) and the imaging features of the nodule can help to narrow the differential diagnosis and estimate the probability of malignancy. The patient in this question is a young never smoker with a sizable solid rounded nodule. Her presenting symptoms of bronchitis were not clearly related to the lung nodule, and she did not have a history of prior malignancy, systemic inflammatory conditions, immune suppression, or worrisome exposures. She had a single nodule without related adenopathy. She had not undergone prior imaging to assess the rate of growth of the nodule. This presentation makes many of the potential lung nodule etiologies much less likely but does not lead to one certain diagnosis. Concern for a carcinoid tumor led to her lung resection.1
Fungal infections may present as solid lung nodules in endemic areas, at times with adjacent smaller nodules and regional adenopathy. They will usually be associated with granulomatous inflammation on biopsy (Figure 5), which was not seen in this patient (choice B is incorrect).1
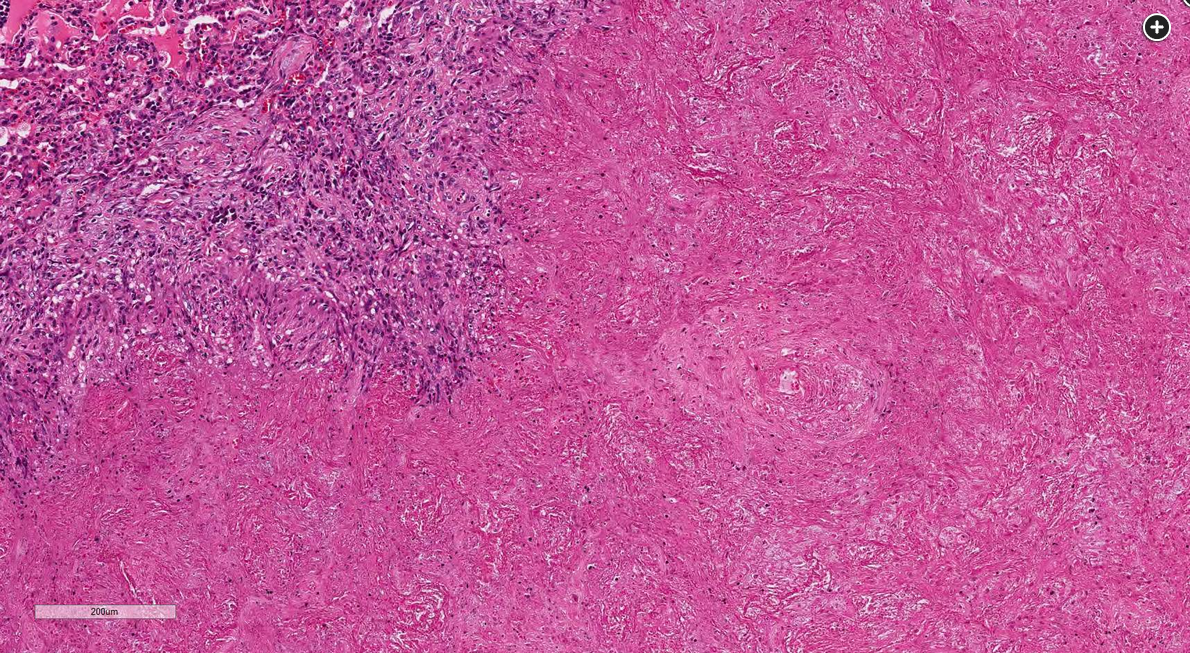
- Figure 5. H&E stain, ×40 magnification.