inferior MI could be right sided STEMI
- related: Cardiology and Hemodynamics
- tags: #literature #icu #cardiology
- suspect RV infarction in all inferior MI (although only happens in 30% patients)
- clinical signs: JVD, hypotension, clear lungs
- significance: RV infarct can lead to decreased LV preload
- avoid excessive fluid that can further move septum to left
- avoid nitroglycerin 123
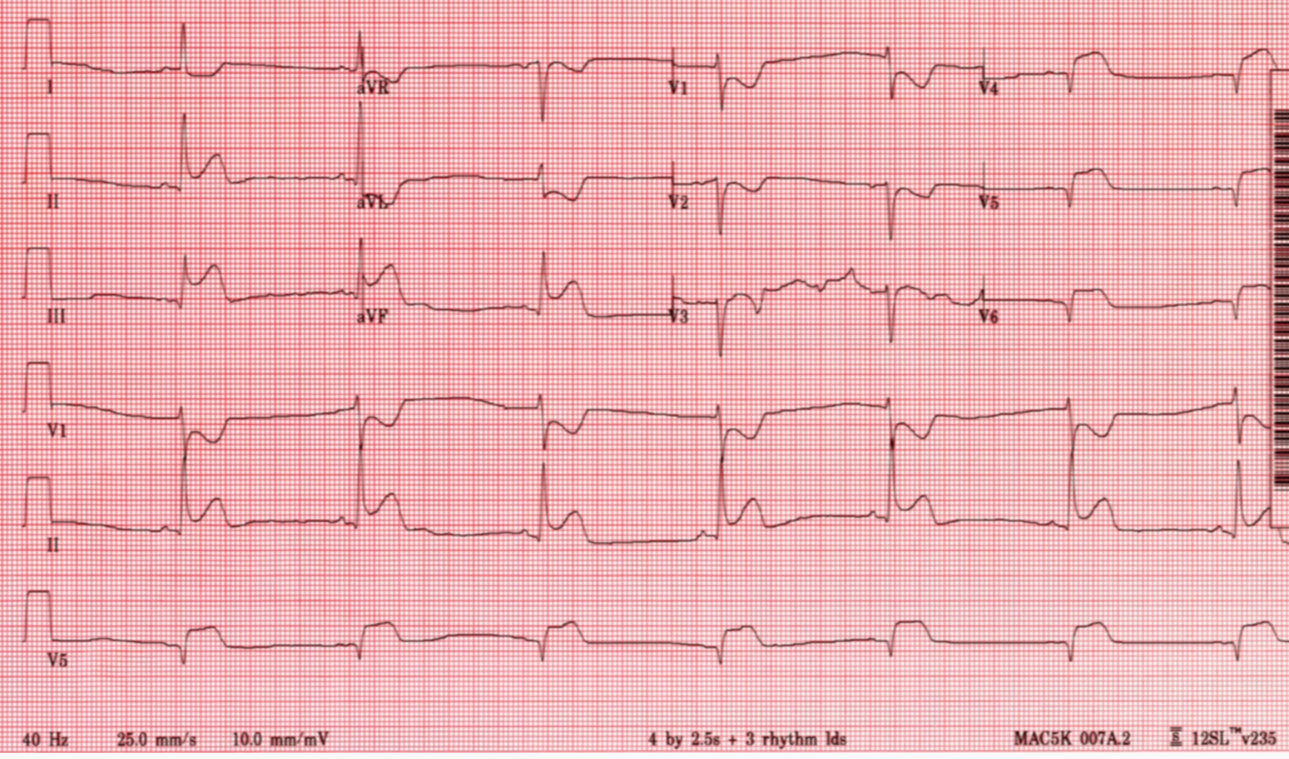
Hypotension in a patient with an acute inferior wall myocardial infarction (MI) should raise the suspicion of concomitant right ventricular (RV) infarction. This is especially true when profound hypotension occurs after administration of nitroglycerin. The clinical picture of RV infarction reflects the hemodynamic situation and includes elevated right-sided pressures with normal or low left-sided pressures, as in this case. RV stroke volume is dependent on adequate preload, so a vasodilator such as nitroglycerin can decrease right-sided cardiac output and compromise left ventricular preload as well, causing a decrease in BP (choice C is correct). Identification of RV infarction in a patient with hypotension is important because this is a potentially reversible cause of cardiogenic shock. Vagal activation in inferior MI (Bezold-Jarisch reflex) may lead to diaphoresis and/or vomiting (as well as bradycardia, seen on the presenting ECG), and right-sided pressures may not be greatly elevated, as in this case. This emphasizes the need for a high index of suspicion of RVMI in patients with inferior infarction. The diagnosis can be made by obtaining an ECG with right-sided chest leads; more than 1 mm of ST elevation in leads V4R and/or V5R is a specific sign. In addition, ST depression in leads V1 to V3 reciprocal to the inferior ST elevation, as seen in this presenting ECG, increases the suspicion of RV infarction, although this is not an especially specific sign.
The diagnosis can also be made by echocardiography, with demonstration of RV hypokinesis. Echocardiography can also be used to rule out other causes of hypotension in acute MI. Acute ventricular septal rupture or mitral regurgitation from papillary muscle rupture would most likely have a cardiac murmur and would present with pulmonary edema (choices B and D are incorrect). Cardiogenic shock due to left-sided pump failure would also present with pulmonary congestion (choice A is incorrect).
Initial treatment of RV infarction involves administration of fluids, although an attempt should be made to avoid overdistension of the right ventricle, which can shift the interventricular septum to the left and thus decrease left ventricular filling. If this is suspected, echocardiography can be useful to evaluate chamber dimensions. Patients who remain hemodynamically unstable after fluids may respond to inotropic therapy. Patients failing to respond may be candidates for right-sided mechanical support, although this is not usually necessary.456
A 71-year-old man presents with nausea, vomiting, diaphoresis, and chest pressure. His BP is 110/65 mm Hg, heart rate is 46/min, respirations are 16/min, and temperature is 37.5°C. His jugular venous pressure is 12 cm H2O, and his lungs are clear. Cardiac examination is unremarkable. His presenting ECG is shown in Figure 1. He is given sublingual nitroglycerin and 5 min later becomes confused. His systolic BP is palpated at 65 mm Hg. His heart rate is 50/min. The rest of the physical examination is unchanged. The most likely cause of this patient’s decompensation is which of the following?
Links to this note
-
anterior ST depression is either anterior ischemia or posterior STEMI
- caution with nitrates use for possible inferior MI could be right sided STEMI
Footnotes
-
Dell’Italia LJ, Starling MR, Blumhardt R, Lasher JC, O’Rourke RA. Comparative effects of volume loading, dobutamine, and nitroprusside in patients with predominant right ventricular infarction. Circulation. 1985;72(6):1327-1335. PubMed ↩
-
Jacobs AK, Leopold JA, Bates E, et al. Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry. J Am Coll Cardiol. 2003;41(8):1273-1279. PubMed ↩
-
Jacobs AK, Leopold JA, Bates E, et al. Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry. J Am Coll Cardiol. 2003;41(8):1273-1279. PubMed ↩
-
Kapur NK, Esposito ML, Bader Y, et al. Mechanical circulatory support devices for acute right ventricular failure. Circulation. 2017;136(3):314-326. PubMed ↩
-
Moye S, Carney MF, Holstege C, et al. The electrocardiogram in right ventricular myocardial infarction. Am J Emerg Med. 2005;23(6):793-799. PubMed ↩