renal artery stenosis can cause recurrent flash pulmonary edema
- related: Nephrology
- tags: #nephrology #literature #pulmonology
This patient is experiencing her second episode of flash pulmonary edema associated with severe hypertension. She has peripheral arterial disease (intermittent claudication) and multiple risk factors (smoking, diabetes, hyperlipidemia) for diffuse atherosclerosis. Recurrent flash pulmonary edema in patients with atherosclerotic disease should raise suspicion for renovascular hypertension due to bilateral renal artery stenosis.
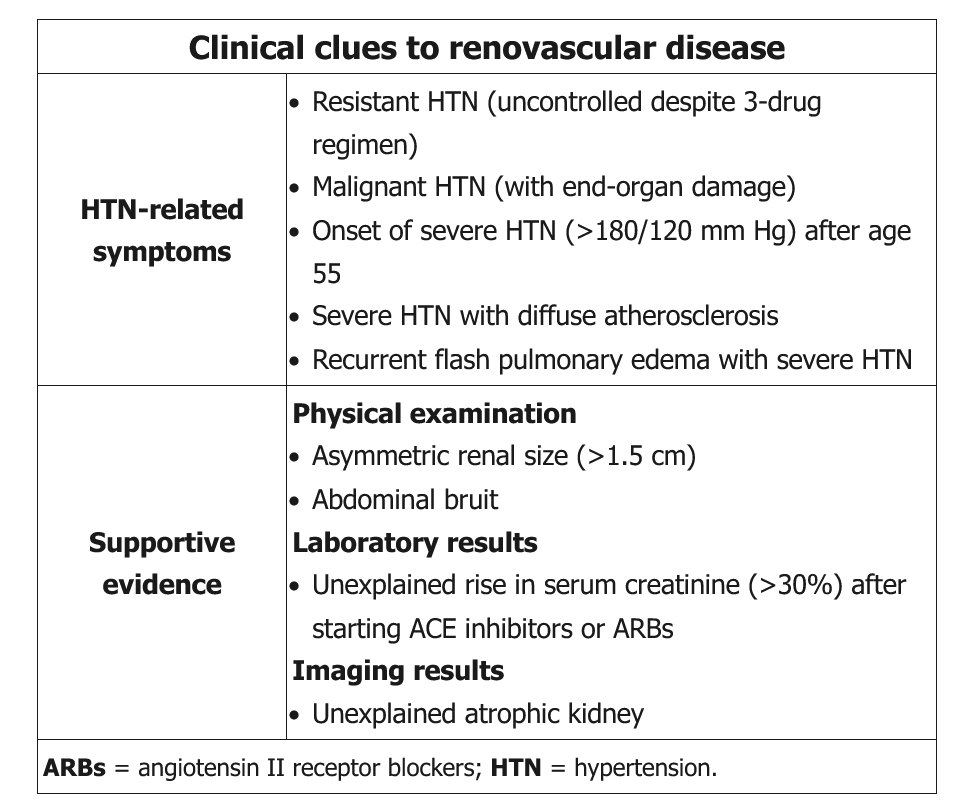
Patients with bilateral renal artery stenosis can experience flash pulmonary edema (Pickering syndrome) despite normal left ventricular ejection fraction. Other clues for renovascular hypertension include an acute rise in serum creatinine (>30%) after initiation of an ACE inhibitor or unexplained renal asymmetry on imaging studies. Patients who have a high likelihood of renovascular disease should be evaluated with renal Doppler ultrasound or CT or MR angiography to detect renal artery stenosis.1
The patient’s extensive smoking history and hypertension would be reasons to suspect he has severe atherosclerotic disease for which renovascular disease and other cardiovascular risks are well correlated. Recurrent flash pulmonary edema would further support this (choice C is correct).
In patients with coronary artery disease, some degree of renovascular disease can be seen in 10%, as opposed to less than 1% of patients with primary hypertension. In addition to severe hypertension in patients with diffuse atherosclerosis, renal artery stenosis should be considered if the patient has secondary hypertension with sudden severe onset of more than 180/120 mm Hg and is older than 55 years, has deterioration of renal function while receiving an angiotensin-converting enzyme or an angiotensin-receptor blocker, has radiographic evidence of renal atrophy, has recurrent flash pulmonary edema, and has an abdominal bruit. Testing can include contrast-enhanced magnetic resonance angiography, CT angiography, or Doppler ultrasonography.
Hypokalemia is associated with primary hyperaldosteronism, which is another common cause of secondary hypertension in patients with refractory disease. The potassium is wasted in the urine, and the diagnosis can be made by evaluating the aldosterone:renin ratio to determine whether the aldosterone level is inappropriately high for the renal level (choice A is incorrect).
Daytime somnolence as well as fatigue, morning confusion, and difficulty concentrating are signs of OSA. Although OSA is frequently associated with hypertension, this degree of hypertension would not likely be associated with OSA alone (choice B is incorrect).
Headache is not commonly associated with renal artery stenosis, but it is a common finding with OSA, which is another common potential cause of secondary hypertension. Headache can also be seen in pheochromocytoma, which would be an uncommon cause of secondary refractory hypertension (choice D is incorrect).2