STEMI treatment
- related: Cardiology and Hemodynamics
- tags: #literature #cardiology
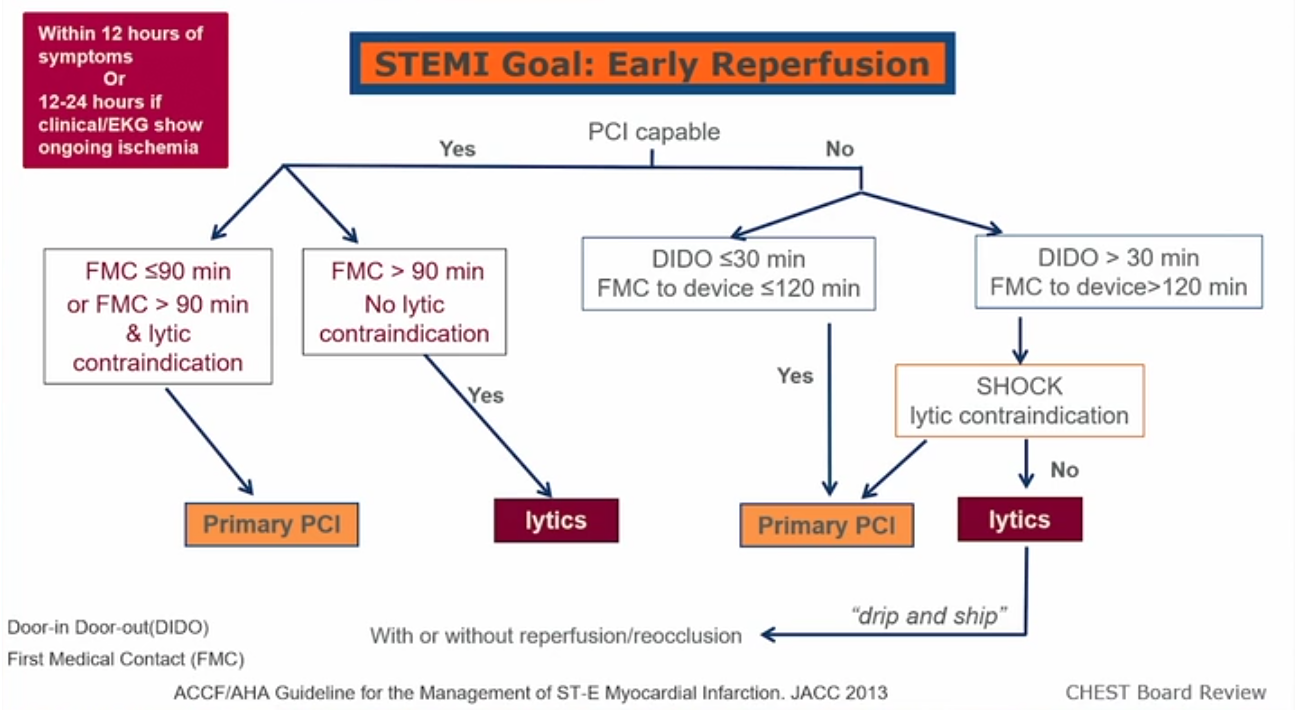
- Either PCI or fibrinolytic is appropriate for patients with symptom onset < 12 hours with no contraindication
- PCI is better at restoring blood flow when it can be done fast enough
- Door to balloon time: 90 minutes
- If no PCI is available, consider transfer if can achieve contact to PCI in 120 minutes
- Door to needle (tpa) time: 30 minutes
- Door to departure time for places without either: 30 minutes1
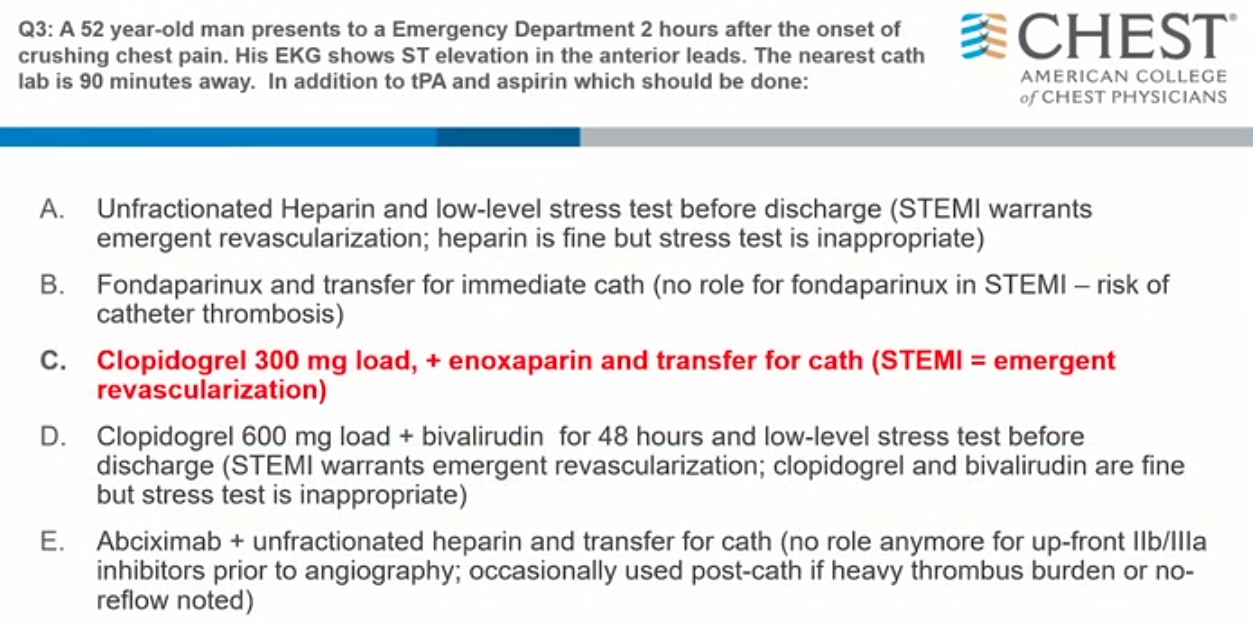
- Clopidogrel + any heparin + transfer
- Aim is: 2 hours (200 minutes) from presentation to artery open is when delay in care is not ok
- If hospital has capability: open in 90 minutes (1.5 hours)
- if hospital has no primary PCI
- if far away: lytics in 30 minutes
- if close by: 30 minutes at referring, 60 minutes transfer, 30 minutes to do cath. Acceptable transfer delay is 60 minutes between hospitals
- ticagrelor or prasugrel are superior than clopidogrel in terms of antiplatelet but higher bleeding risk
- PCI capable: very rare to do lytics. Pretty much only if there’s no physical room
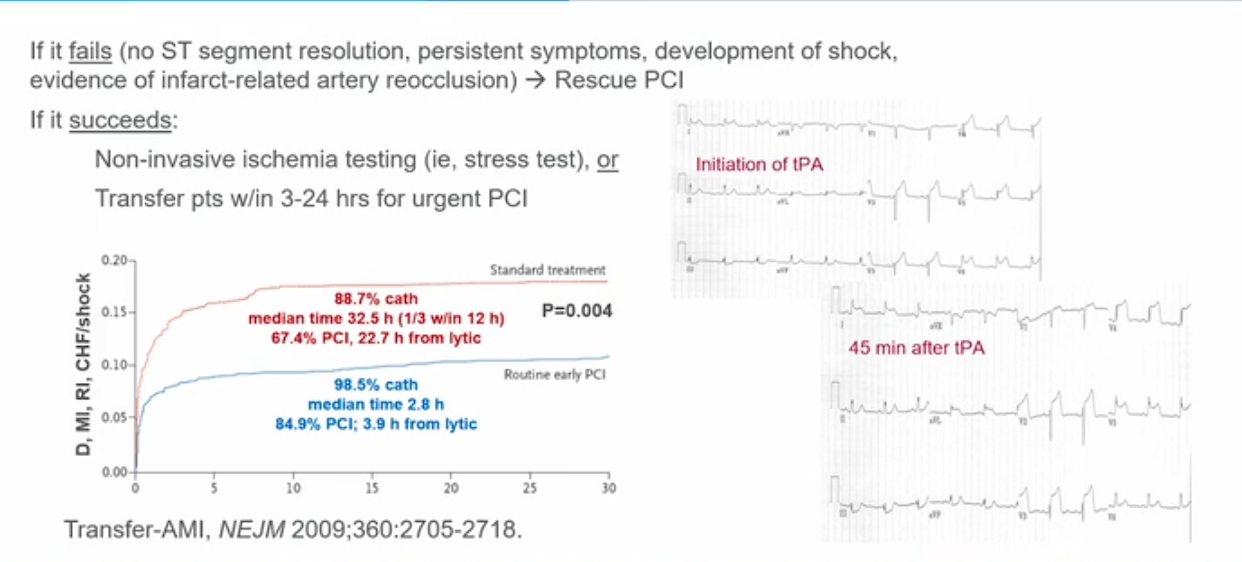
- at 45 minutes mark, if there is no 50% decrease in ST elevation and still has symptom, that means rescue PCI is needed
- Basically, lytics and transfer. Patient will get PCI even after lytics
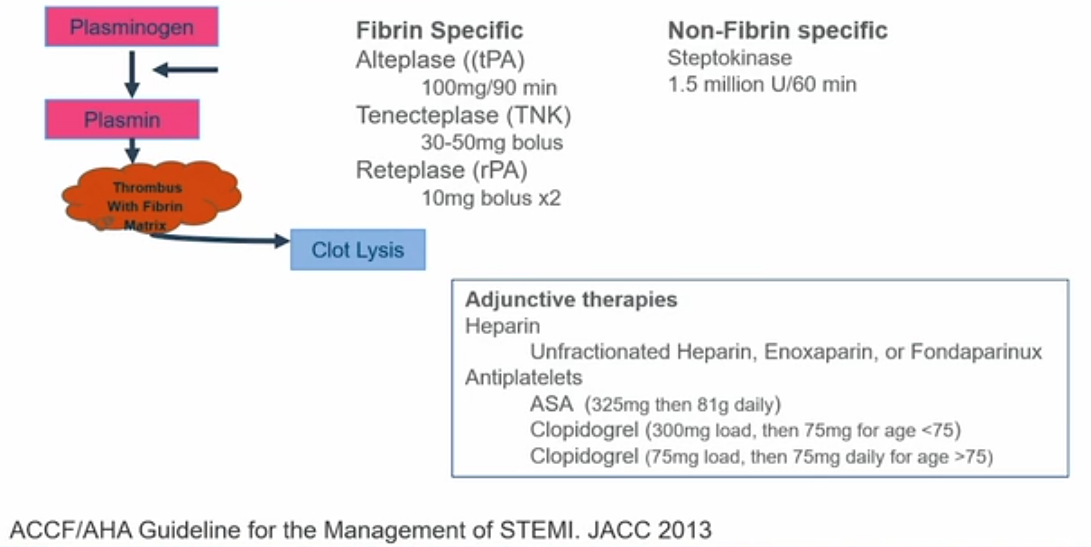
- every one with lytics also gets heparin (different from stroke), antiplateletes
Links to this note
Footnotes
-
ACLS Heart Code ↩