toxic leukoencephalopathy
- related: Neurology
- tags: #literature #neuro
Toxic leukoencephalopathy is a disorder of brain white matter caused by exposure to leukotoxic agents. These leukotoxins include therapeutic drugs, drugs of abuse, and environmental insults. A method of inhalation opioid abuse that involves heating opioid over aluminum foil and inhaling opioid fumes is a well-known cause of toxic leukoencephalopathy and is the most likely cause of this patient’s rapidly progressive neurologic disorder (choice C is correct).
The opioid epidemic is a massive public health crisis, and, although IV opioid use remains most common, inhalation is a rapidly increasing route of use. Opioid fume inhalation (sometimes referred to as “chasing the dragon”) involves heating heroin, or fentanyl, over aluminum foil with a controlled flame and using a tube to inhale the fumes and “chase” after the vapor. The inhaled route has a safer infectious profile compared with IV routes, but inhalational abuse is associated with toxic leukoencephalopathy, which is a devastating neurologic complication (as seen in this patient’s case). It has been hypothesized that aluminum toxicity causes the leukoencephalopathy associated with this particular method of opioid inhalation; however, this hypothesis has not been confirmed and remains controversial.
The toxic leukoencephalopathy from opioid fume inhalation is typically classified into three severity levels based on neurologic impairments: (1) mild: inattentiveness, confusion, ataxia, and psychomotor symptoms; (2) moderate: corticospinal or extrapyramidal involvement and impaired levels of alertness ranging from severe confusion to delirium; and (3) severe: generalized motor impairment, abulia without language disorders or apraxia, noticeable alertness deficits, and, in many patients, progression to death. There is no treatment-specific management for this toxic leukoencephalopathy. MRI findings of this toxic leukoencephalopathy include restricted diffusion in both globi pallidi and the cerebellum accompanied by symmetric hyperintensities on T2-weighted and fluid-attenuated inversion recovery images. The most common findings are bilateral, symmetric, periventricular white matter reduced diffusion, characteristically with symmetric involvement of white matter (the cerebellum and the posterior limb of the internal capsule). The injury is most severe in the cerebellum and cerebral hemispheres, superior cerebellar peduncle, tractus solitarius, and medial lemniscus.
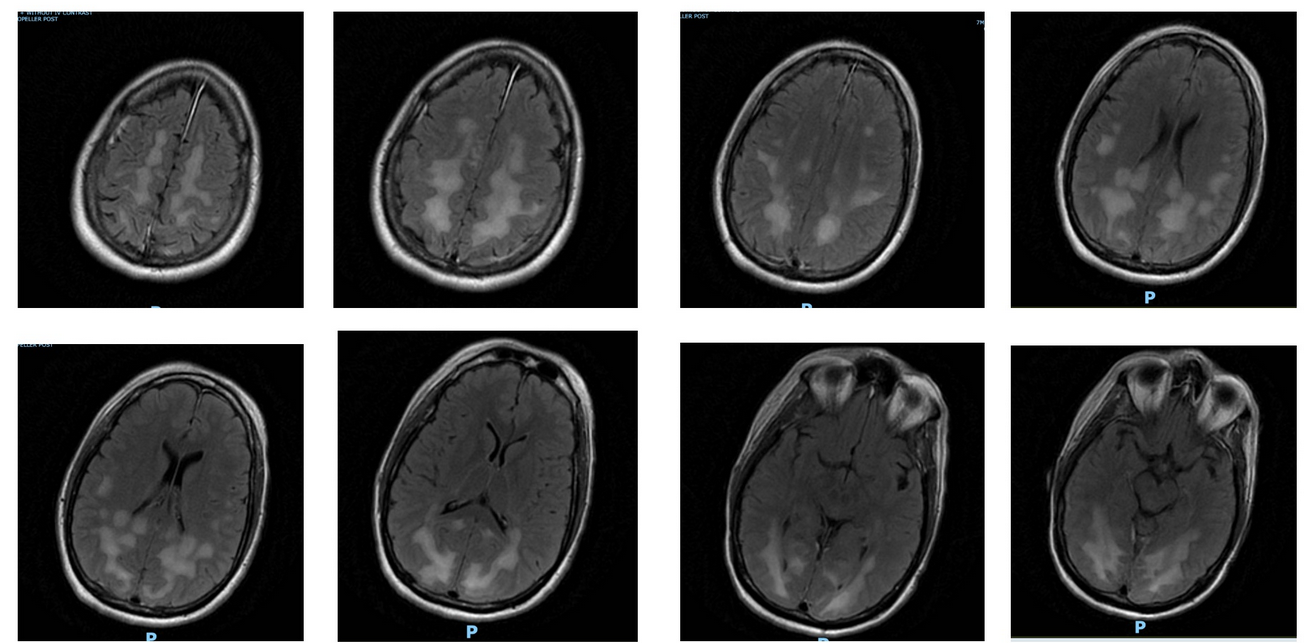
T2-weighted fluid-attenuated inversion recovery images from MRI performed using a multisequence, multiplanar technique with and without IV contrast material.
Progressive multifocal leukoencephalopathy (PML) is caused by the reactivation of polyomavirus JC (John Cunningham virus). It is a rare disease that almost exclusively affects patients who are immunocompromised, including recipients of organ transplants, patients with HIV, or individuals receiving chronic corticosteroids. PML typically manifests with subacute neurologic abnormalities (choice A is incorrect).
Posterior reversible encephalopathy syndrome (PRES) is most commonly described in patients with hypertensive encephalopathy and/or the use of immunosuppressants, and the typical MRI findings in PRES include white matter edema in the posterior cerebral hemispheres. The MRI findings in this case are classic for chasing the dragon and less suggestive of PRES (choice B is incorrect).
Herpes simplex encephalitis often manifests with seizures, and MRI findings classically involve the temporal lobe. This patient was without seizures on cEEG and lumbar puncture, and his MRI findings are not consistent with herpes simplex encephalitis (choice D is incorrect).1234
A 28-year-old patient with a history of polysubstance use disorder (alcohol, cocaine, opioids) was brought into the emergency department by his roommate who found him engaging in violent, self-harm behavior. His roommate reports that the patient had been in his usual state of health until 2 days ago when he reported “feeling odd” after inhalation of an unknown substance.
His vital signs at presentation include a temperature of 37 °C, heart rate of 124/min, BP of 151/88 mm Hg, respiratory rate of 27/min, and SpO2 of 98% while breathing ambient air. On neurologic examination, he is alert and oriented to self, follows simple commands, but is inattentive. His voice is hypophonic, his speech is often incoherent, and he has evidence of occipital blindness on examination. He does not move his upper extremities, even to painful stimuli, and has limited movement in his lower extremities. Sensation to light touch and pain is intact. Emergency head CT scan reveals widespread cerebral and cerebellar white matter hypodensities and no intracranial hemorrhage. Lumbar puncture results demonstrate an RBC count of 2,000/µL (0.002 × 1012/L), WBC count of 11,000/µL (11 × 109/L), glucose level of 104 mg/dL (5.77 mmol/L) (serum, 129 mg/dL [7.16 mmol/L]), and protein level of 51 mg/dL; herpes simplex virus (HSV)-1 and HSV-2 polymerase chain reaction results are negative; Gram stain and culture results are negative; and Venereal Disease Research Laboratory (VDRL) screen results are nonreactive. Urine drug screening results are positive for opioids. Results from a comprehensive metabolic panel are all within normal limits. A 72-h continuous EEG does not show seizures. Results from MRI of the brain are shown in Figure 1.
Over the next 2 weeks, his examination results progressively worsen to the point that he is minimally responsive but spontaneously opens his eyes. When his head is touched, his arms display extensor posturing.
What is the most likely cause of this patient’s clinical presentation and trajectory?
Links to this note
Footnotes
-
Alambyan V, Pace J, Miller B, et al. The emerging role of inhaled heroin in the opioid epidemic: a review. JAMA Neurol. 2018;75(11):1423-1434. PubMed ↩
-
Cortese I, Reich DS, Nath A. Progressive multifocal leukoencephalopathy and the spectrum of JC virus-related disease. Nat Rev Neurol. 2021;17(1):37-51. PubMed ↩
-
Keogh CF, Andrews GT, Spacey SD, et al. Neuroimaging features of heroin inhalation toxicity: “chasing the dragon.” AJR Am J Roentgenol. 2003;180(3):847-850. PubMed ↩