urine anion gap differentiates between GI vs renal causes of NAGMA
- related: Nephrology
- tags: #literature #nephrology
The urine anion gap, which is the urine sodium level plus the urine potassium minus the urine chloride levels, can be used to differentiate between GI and renal causes of normal gap metabolic acidosis. A normal urine anion gap is 0 or slightly positive. Normal functioning kidneys excrete acid through ammonium (NH4+). Chloride (Cl-) is the anion that is excreted along with that ammonium cation. The urine of a patient with acidosis and normally functioning kidneys will have increased ammonium cations (and therefore increased chloride anions) in the urine to try to excrete the increased acid in the body. This increase in chloride anions in the urine will make the urine anion gap negative. When the kidneys are functioning properly, the urine anion gap will be negative in a patient with hyperchloremic metabolic acidosis. In this patient, the urine anion gap is –17 (31 + 12 – 60 = –17), suggesting a GI cause for the normal anion gap hyperchloremic metabolic acidosis.
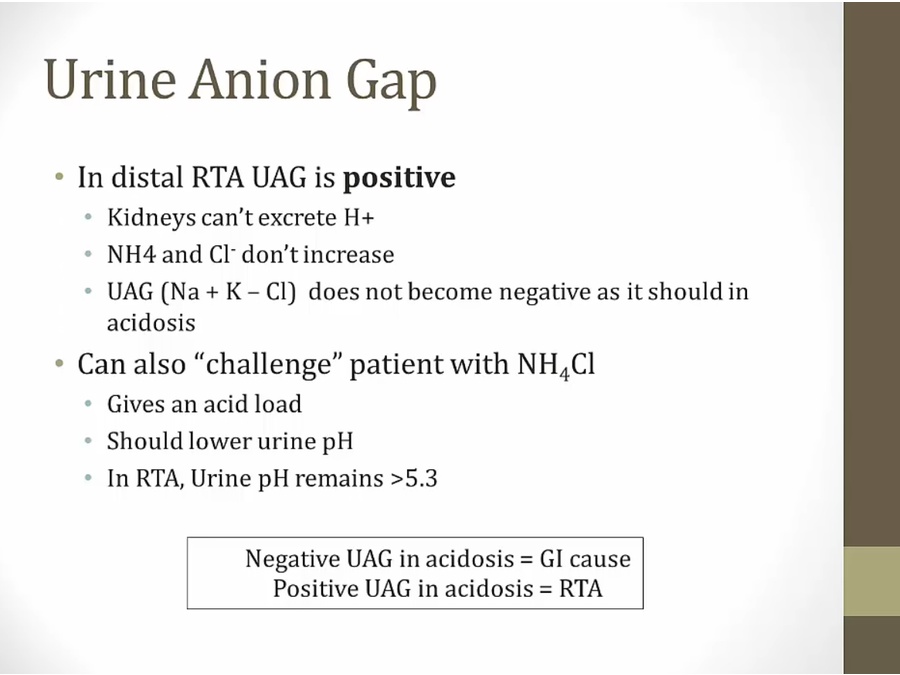
The patient clearly has risk factors for developing renal tubular acidosis (RTA). She has new, acute renal failure and takes a number of medications that can cause type 4 RTA, including angiotensin-converting enzyme inhibitors and spironolactone. The primary problem in type 4 RTA, however, is lack of aldosterone effect on the kidney, either through decreased aldosterone secretion or aldosterone resistance. This lack of aldosterone effect on the kidney leads to hyperkalemia, which is characteristic of type 4 RTAs and which she does not have. In addition, when the normal gap acidosis is due to RTA, the malfunctioning kidneys have impaired secretion of ammonium cations (and thus chloride anions). In these situations, the urine chloride level remains relatively low, and the urine anion gap is positive.123456
In RTA, the kidney is unable to excrete NH4+ and Cl-, thus UAG is positive.
- urinary anion gap equation different from plasma anion gap
- urine Cl goes up, UAG becomes negative
Links to this note
Footnotes
-
Batlle DC, Hizon M, Cohen E, et al. The use of the urinary anion gap in the diagnosis of hyperchloremic metabolic acidosis. N Engl J Med. 1988;318(10):594-599. PubMed ↩
-
Emmett M, Narins RG. Clinical use of the anion gap. Medicine (Baltimore). 1977;56(1):38-54. PubMed ↩
-
Gabow PA, Kaehny WD, Fennessey PV, et al. Diagnostic importance of an increased serum anion gap. N Engl J Med. 1980;303(15):854-858. PubMed ↩
-
Kraut JA, Madias NE. Serum anion gap: its uses and limitations in clinical medicine. Clin J Am Soc Nephrol. 2007;2(1):162-174. PubMed ↩
-
Uribarri J, Oh MS. The urine anion gap: common misconceptions. J Am Soc Nephrol. 2021;32(5):1025-1028. PubMed ↩