acute abdominal compartment syndrome
- related: Nephrology, ICU intensive care unit
- tags: #nephrology #icu #literature
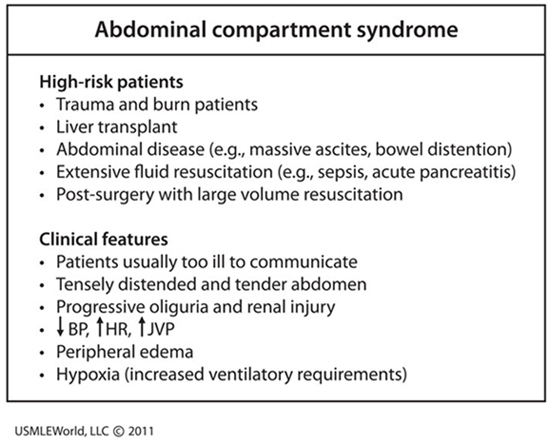
This patient’s presentation is consistent with likely intra-abdominal hypertension (IAH) causing abdominal compartment syndrome (ACS). Intra-abdominal hypertension is defined as pressure > 12 mm Hg; and ACS is defined as IAH with new organ dysfunction. Primary ACS is due to abdominal pelvic disease, while secondary ACS is usually due to extra-abdominal conditions (e.g., burns). Abdominal compartment syndrome occurs in patients receiving large amounts of fluids and almost any organ can be affected (especially the kidney due to its anatomical position).
While the exact pathophysiology is unknown, acute kidney injury is likely due to decreased renal blood flow and elevated renal venous pressure. A diagnosis of ACS can rapidly be confirmed by measuring hydrostatic pressure within the bladder, which is strongly correlated with intra-abdominal pressure. Lowering intra-abdominal hydrostatic pressure often quickly improves renal function; however, most patients require surgical decompression. Abdominal compartment syndrome has a mortality rate ranging as high as 40-100%.
Abdominal compartment syndrome is defined as a sustained intra-abdominal pressure (IAP) >20 mm Hg associated with at least one organ dysfunction. Abdominal compartment syndrome occurs in the setting of abdominal surgery, trauma, hemoperitoneum, retroperitoneal bleed, ascites, bowel obstruction, ileus, and pancreatitis. It can also occur from capillary leak from massive fluid resuscitation or sepsis. Increasing IAP causes hypoperfusion and ischemia of the intestines and other peritoneal and retroperitoneal structures, leading to hemodynamic, respiratory, neurologic, and kidney impairment. Renal vein compression and renal artery vasoconstriction cause oliguric AKI.
Abdominal compartment syndrome is diagnosed by measuring IAP; measurement of bladder pressure with an indwelling catheter is the standard methodology. Management includes supportive therapy, abdominal compartment decompression, and correction of positive fluid balance.
The respiratory system mechanics in this patient indicate an extremely low compliance circumstance. In this clinical context, it is likely due to an abdominal compartment syndrome (ACS) complicating the patient’s pancreatitis. Measuring the bladder pressure as a surrogate of the abdominal pressure will make a diagnosis, determine the severity, and guide interventions (choice B is correct).
Measuring the respiratory system mechanics during mechanical ventilation is extremely useful to elucidate causes of respiratory failure. In this patient not making active efforts to breathe, the respiratory system compliance is equal to the tidal volume divided by the inflating pressure (plateau airway pressure minus the PEEP). Since the tidal volume is relatively small, and the inflating pressure very high (44 cm H2O), the respiratory system compliance is very low. That could result from the lungs themselves being stiff, but with only moderately impaired gas exchange and absence of dense infiltrates on the chest radiograph, extremely severe lung injury with diminished compliance, as seen in ARDS, is not likely. Accordingly, the cause of low compliance here is likely the chest wall (including the abdominal compartment). When this patient’s bladder pressure was measured, it was 25 mm Hg. Surgical consultation was obtained and when the bladder pressure continued to climb in the ensuing hours, the patient was taken for a decompressive laparotomy.
ACS refers to the development of abdominal hypertension that in turn leads to multiple organ failure. It is caused by many conditions encountered in the ICU, including trauma, burns, obstetric catastrophes, liver transplantation, pancreatitis, post-operative complications, and sepsis. Intra-abdominal hypertension (IAH) is defined as sustained pressures >12 mm Hg (16 cm H2O) with severe IAH (grade IV) indicated by pressures >25 mm Hg (34 cm H2O). A more useful measurement is the mean blood pressure minus the intra-abdominal pressure since this is a reflection of the perfusing pressure of the viscera. When this pressure falls below 60 mm Hg, the possibility of liver, gut, pancreatic, and renal hypoperfusion exists with a downward spiral of organ function and eventual death. Patients with high intra-abdominal pressures, lactic acidosis, diminished perfusing pressure of the abdominal compartment, and multiple organ failure require early identification and a rapid intervention to reduce abdominal pressure. Decompressive laparotomy is often required to halt this process.
Intra-abdominal pressure can be measured indirectly using intragastric, intracolonic, intravesical, or inferior vena cava manometry but measurement of intravesical pressure from an indwelling catheter is most widely employed. Protocols should be established in all ICUs to make this measurement readily and reliably given the wide range of conditions that may produce ACS.
Measuring right atrial pressure would not particularly guide management of a patient with ACS (choice A is incorrect), but a suggestion of the presence of IAH is sometimes seen on a central venous pressure tracing since the intra-thoracic pressure can rise precipitously with each breath delivered by the ventilator, as shown in Figure 1. Measurement of esophageal pressure has been advocated by some to help determine the actual transpulmonary pressure in patients with confounders preventing airway pressure from accurately reflecting lung mechanics alone (eg, obesity, intra-abdominal processes) but it is more cumbersome than measurement of bladder pressure, and it would not directly assess the magnitude of IAH and the need to address it (choice C is incorrect). End tidal CO2 monitoring should be used in most patients undergoing mechanical ventilation but it would not give useful information regarding ACS (choice D is incorrect).
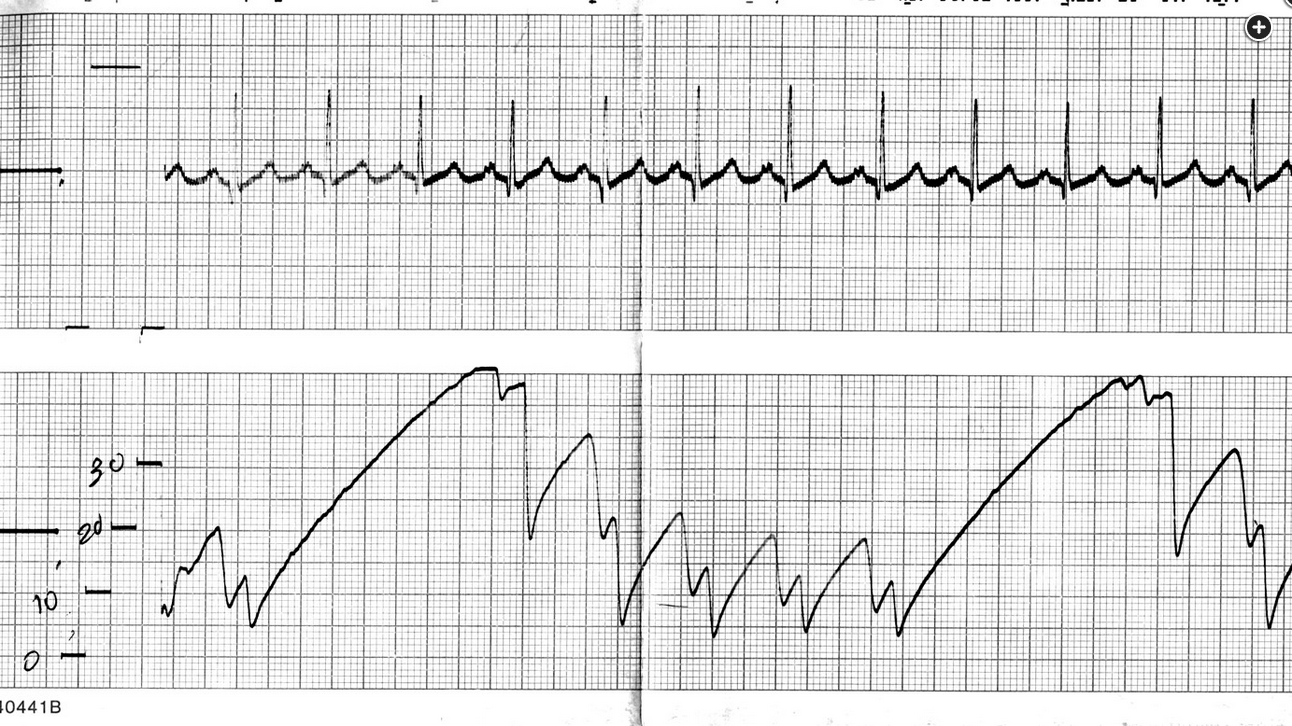
Right atrial pressure tracing in a patient with pancreatitis and abdominal compartment syndrome. Note the relatively high baseline pressure climbs to extremely high levels with each inspiration.
Acute abdominal compartment syndrome is a rare but dreaded complication of abdominal surgeries (Figure 1). It occurs in 10% to 30% of patients who are nontraumatically injured and critically ill. Intraabdominal pressure (IAP) is defined by the end-expiratory pressure in the abdomen in the supine position in a fully relaxed patient. Abdominal perfusion pressure is the difference between the mean arterial pressure and IAP. A sustained IAP greater than 12 mm Hg is diagnostic of intraabdominal hypertension. Physiologic consequences of intraabdominal hypertension include clinical signs of impeded venous return, dangerously elevated pulmonary peak and plateau pressures despite full relaxation, and acute onset oliguria. These signs should raise concern about the development of abdominal compartment syndrome.
Abdominal compartment syndrome is diagnosed with serial bladder pressure measurements under heavy sedation or paralysis. Point-of-care ultrasonography will frequently show free fluid in the abdomen. This is especially true in the postoperative patient or when there has been a large volume resuscitation or underlying cardiac or hepatic failure, but fluid alone is not diagnostic of abdominal compartment syndrome. Serial abdominal examinations are not sensitive enough to diagnose abdominal compartment syndrome. Lactic acid is commonly elevated in patients in shock, and an elevated lactate level is not diagnostic of abdominal compartment syndrome.
To obtain bladder pressure, follow these recommended steps. Insert a urinary catheter and allow urine drainage, then prepare an arterial line setup with a 1-L bag of saline. Connect the three-way stopcock attached to a 60-mL saline syringe to the end of the arterial line tubing. Have the patient lie flat, and connect the three-way stopcock to the urinary catheter access port. At the level of the iliac crest in the midaxillary line, zero the pressure transducer. By using forceps, clamp the drainage bag of the urinary catheter just distal to the culture aspiration.
Next, via the three-way stopcock, instill 60 mL of sterile saline into the bladder. Turn the stopcock off to the syringe. Upon completion, open to the patient. Briefly unclamp the distal urinary catheter to allow all air in the proximal collection tubing to pass into the distal tubing and then reclamp. Allow 60 s for detrusor muscle relaxation before obtaining measurements. Record the measurement when you have a solid waveform. The bladder pressure should be measured at the end of exhalation with the patient completely flat in the supine position. Unclamp the urinary catheter and remove the pressure transducing tubing. Subtract 60 mL from the total urine output if strict measurement of urine output is necessary for the patient. If the patient is not adequately sedated or paralyzed when the measurements are obtained, the results can be spurious and unreliable.
Abdominal compartment syndrome with intraabdominal hypertension greater than 25 mm Hg on bladder pressure measurement should be treated with decompressive laparotomy (choice D is correct). The use of sedatives to achieve a Richmond Agitation-Sedation Scale score of -3 and administration of neuromuscular blockade during bladder pressure measurement are typically necessary to obtain accurate measurements, but this intervention will not therapeutically address this patient’s rapidly deteriorating clinical condition (choice A is incorrect).
Paracentesis is generally used in patients with large-volume ascites when there is a concern for primary or secondary peritonitis, and in the context of abdominal compartment syndrome, large-volume paracentesis can reduce the pressure inside the abdomen. However, the underlying cause must be treated or the volume will reaccumulate. Among patients with chronic ascites associated with cardiac and hepatic failure, the abdominal wall is able to accommodate and stretch without causing intraabdominal compartment syndrome. However, this patient does not have a clinical history to suggest chronic ascites to explain her distended abdomen. Furthermore, paracentesis is unlikely to reverse the cause of the intraabdominal hypertension, and decompressive laparotomy should not be delayed for this procedure (choice B is incorrect).
Decompression of the GI tract with nasogastric tube and rectal tube placement are helpful maneuvers in patients with ileus or pseudo-obstruction from critical illness. Many patients with abdominal compartment syndrome have an ileus. Decompressing the GI tract is helpful to ensure the ileus resolves nonoperatively by reducing the diameter of the bowel, decreasing pressure intraluminally, and therefore reducing risks of bowel perforation. However, if a patient has true abdominal compartment syndrome on the basis of the clinical scenario, including the history, accompanying physiologic derangements and intraabdominal hypertension greater than 20 mm Hg, decompression of the GI tract alone will not suffice (choice C is incorrect).

This patient has developed abdominal compartment syndrome (ACS) in the setting of severe pancreatitis and aggressive volume resuscitation (10 L of crystalloid fluid) in the first 24 h (choice C is correct). ACS is a significant cause of morbidity and mortality in critically ill patients, and early detection is critical. ACS requires both an elevated intraabdominal pressure (IAP) and new organ dysfunction resulting from elevated IAP. More specifically, the World Society of the Abdominal Compartment Syndrome (WSACS) defines intraabdominal hypertension (IAH) as an IAP ≥12 mm Hg and ACS as a sustained IAP ≥20 mm Hg with new organ dysfunction or failure. The WSACS also created severity grades for IAH (grade I, IAP 12-15 mm Hg; grade II, IAP 16-20 mm Hg; grade III, IAP 21-25 mm Hg; and grade IV, ≥25 mm Hg). Bladder pressure measurements should be obtained when the patient is in the complete supine position without evidence of abdominal muscle contractions.
ACS is classified as primary or secondary. Primary ACS is due to intraabdominal and/or retroperitoneal processes, such as blunt or penetrating trauma, hemorrhage, abdominal aortic aneurysm rupture, and retroperitoneal hemorrhage. Secondary ACS is due to bowel edema or tense ascites in patients with capillary leak syndrome who undergo massive fluid resuscitation. Common causes of secondary ACS include sepsis, pancreatitis, hemorrhagic shock, and burns. The physiological consequences of IAH and ACS affect the pulmonary, cardiovascular, renal, GI, and hepatic systems and CNS. Increased IAP displaces the diaphragm cephalad, increasing intrathoracic pressure and decreasing dynamic pulmonary compliance, which results in increased peak and plateau pressures. Increased IAP also leads to increase shunt and dead space ventilation, with resultant decrease in PaO2 and increase in PaCO2, as was seen in this patient. IAH affects the cardiovascular system via direct compression on the heart and compression of the inferior vena cava, resulting in decreased venous return, leading to decreased cardiac output and shock. ACS is often associated with increased pulmonary capillary wedge pressure and elevated central venous pressures (choice B is incorrect). Acute kidney injury from IAH is due to direct renal vein compression and renal artery vasoconstriction, resulting in oliguria and anuria, which are among the earliest signs of increased IAP. Additionally, the intestines appear to be quite sensitive to increases in IAP, with decreases in mesenteric blood flow causing intestinal hypoperfusion and edema, with resultant bowel ischemia and lactic acidosis.
The best treatment for ACS is prevention. Intensivists need to be diligent and avoid excess fluid administration when appropriate. Once ACS develops, initial management should be conservative, which includes placing the patient in the supine position (elevation of the head increases IAP), deep sedation, and trial of neuromuscular blockade. If ACS is in the setting of massive ascites, large-volume paracentesis may decrease the IAH. The definitive management of ACS is surgical decompression through a midline laparotomy, but the effects on mortality have been inconclusive. When troubleshooting the ventilator, one must take note of changes in peak and plateau pressures. The decrease in pulmonary compliance, as demonstrated by an increase in both peak and plateau pressures, is seen in ARDS, cardiogenic pulmonary edema, ACS, obesity, decreased chest wall compliance, and tension pneumothorax.123456
Links to this note
Footnotes
-
An G, West MA. Abdominal compartment syndrome: a concise clinical review. Crit Care Med. 2008;36(4):1304-1310. PubMed ↩
-
Cheatham ML, Malbrain ML, Kirkpatrick A, et al. Results from the International Conference of Experts on intra-abdominal hypertension and abdominal compartment syndrome. II. Recommendations. Intensive Care Med. 2007;33(6):951-962. PubMed ↩
-
De Waele JJ, Hoste EA, Malbrain ML. Decompressive laparotomy for abdominal compartment syndrome—a critical analysis. Crit Care. 2006;10(2):R51. PubMed ↩
-
Doerschug KC, Schmidt GA. Intensive care ultrasound: III. Lung and pleural ultrasound for the intensivist. Ann Am Thorac Soc. 2013;10(6):708-712. PubMed ↩
-
Monnet X, Marik P, Teboul JL. Passive leg raising for predicting fluid responsiveness: a systematic review and meta-analysis. Intensive Care Med. 2016;42(12):1935-1947. PubMed ↩