cerebral T wave inversion is sign of SAH and IPH
- related: Neurology
- tags: #literature #icu #neuro
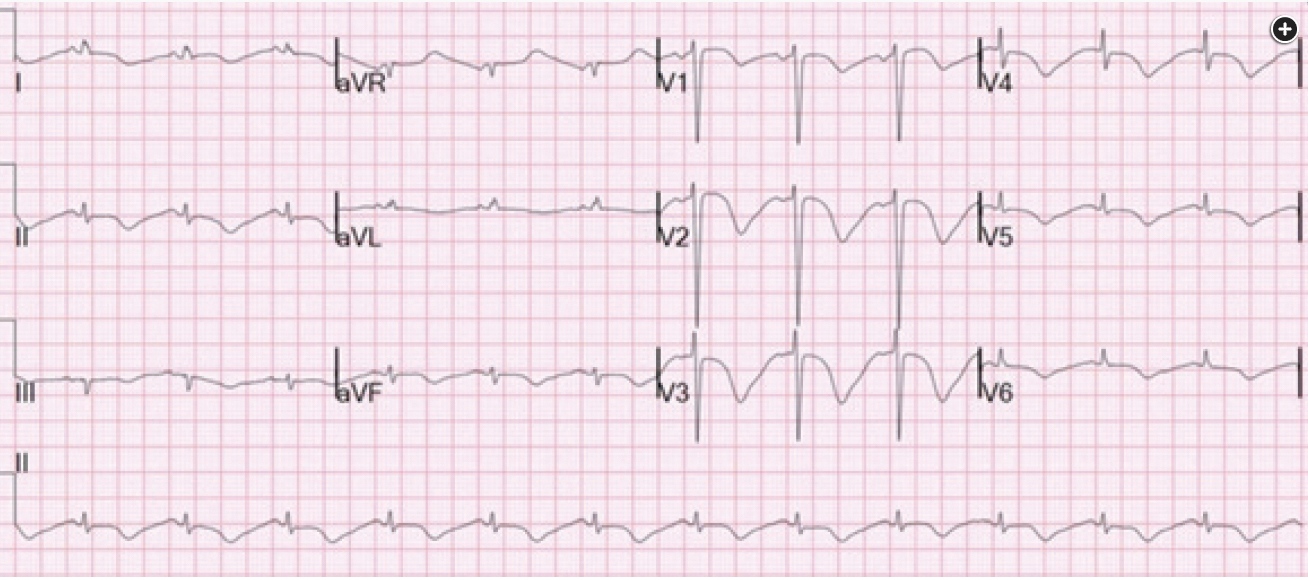
The patient’s ECG demonstrates giant T-wave inversions and QT prolongation. Sometimes known as “cerebral T waves,” these findings correlate with central nervous system (CNS) catastrophes such as subarachnoid hemorrhage (SAH; seen in up to 72% of cases) and intraparenchymal hemorrhage (seen in 57% of cases). Cerebral T waves can also be seen in large ischemic strokes and severe traumatic brain injury. Similar ECG findings can be seen in stress cardiomyopathy and also in profound anterior myocardial ischemia (Wellens syndrome has deep T wave inversion).
SAH accounts for 10% of all strokes and is most commonly caused by a ruptured saccular aneurysm. The patient in this case had multiple risk factors for SAH, including a history of tobacco use and hypertension. Other risk factors include age between 40 and 60 years and a family history of SAH in a first-degree relative, which leads to a threeto fivefold increase in risk over the general population. Classic symptoms of SAH include severe headache, loss of consciousness, and nausea. The most common arrhythmia seen with SAH is either ventricular fibrillation or atrial fibrillation.
In this case, the patient’s history and presentation are highly suggestive of SAH. The stroke guidelines recommend noncontrast-enhanced CT scanning alone to rule out SAH, which has a sensitivity of 90% if performed with a third-generation scanner. Therefore, the best next test in evaluation is noncontrast-enhanced CT scanning of the head, which can quickly help rule out SAH before potential cardiac catheterization (choice C is correct).
Acute pulmonary embolism can be associated with cardiac arrest, but the ECG is not consistent with this diagnosis. Classic ECG findings in pulmonary embolism are sinus tachycardia (most common), T-wave inversions in precordial leads (II, III, and aVF), and nonspecific ST-segment and T-wave changes. The ECG in this patient demonstrates giant T-wave inversions and a prolonged QT interval consistent with CNS catastrophe and not acute pulmonary embolism (choice A is incorrect).
The history and ECG findings are also consistent with either an acute coronary syndrome or stress cardiomyopathy. In fact, “cerebral” T-wave inversion in SAH probably represents stress cardiomyopathy triggered by sympathetic outflow consequent to the SAH in most cases. The clinical presentation of stress cardiomyopathy and acute coronary syndrome can be very similar, as both can include chest pain, ECG changes, and elevated troponin levels; the diagnosis of stress cardiomyopathy entails exclusion of coronary artery disease, usually with coronary angiography. In this case, however, the history is highly suggestive of SAH, and emergent noncontrast-enhanced head CT scanning should be performed quickly. With this level of suspicion for intracranial bleeding, the CT scan should be obtained before administering empiric antiplatelet and/or anticoagulant therapy for suspected acute coronary syndrome (choices B and D are incorrect). If the head CT scanning results are negative, then measurement of serial troponin levels and consideration of cardiac catheterization are reasonable given the cardiac arrest. Echocardiography can be a useful adjunct to other diagnostic measures in this setting as well, with or without a diagnosis of SAH; characteristic wall motion abnormalities may suggest the diagnosis of stress cardiomyopathy and may also elucidate the cause of hypotension, should it be present, as in this case.1234
A 55-year-old woman with a history of essential hypertension, hyperlipidemia, and tobacco use was brought into the emergency department after an out-of-hospital cardiac arrest. The family reports that the patient had had decreased appetite owing to nausea and had complained of headache the night before. While eating dinner, she suddenly lost consciousness and, at further examination, was found to be pulseless. CPR was initiated and continued in the field until emergency medical services (EMS) arrived. When EMS arrived, the patient was in ventricular fibrillation. Epinephrine was administered, and she underwent defibrillation with return of circulation. She was intubated in the field and was brought to the emergency department. At arrival in the emergency department, the patient’s vital signs were as follows: BP, 95/45 mm Hg; heart rate, 85/min; temperature, 34.5 °C; SpO2, 95% with assist-control PEEP of 12 cm H2O; tidal volume, 400 mL; and respiratory rate, 16/min. Her initial ECG is shown in Figure 1.
What diagnostic test should be ordered next?
Links to this note
-
Wellens syndrome has deep T wave inversion
- can look similar to TWI in severe brain injury (cerebral T wave inversion is sign of SAH and IPH)
Footnotes
-
Gregory T, Smith M. Cardiovascular complications of brain injury. Contin Educ Anaesth Crit Care Pain. 2012;12(2):67-71. https://doi.org/10.1093/bjaceaccp/mkr058 ↩
-
Grunsfeld A, Fletcher JJ, Nathan BR. Cardiopulmonary complications of brain injury. Curr Neurol Neurosci Rep. 2005;5(6):488-493. PubMed ↩
-
Hoh BL, Ko NU, Amin-Hanjani S, et al. 2023 Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2023;54(7):e314-e370. PubMed ↩