follicular bronchiolitis
- related: ILD Interstitial Lung Disease or Diffuse Parenchymal Lung Disease
- tags: #literature #pulmonology
- disease: 1.follicular bronchiolitis
- association: 2.Sjogren/RA, immunodeficiency like HIV
- patient and symptoms: 2.older male, gradual sob
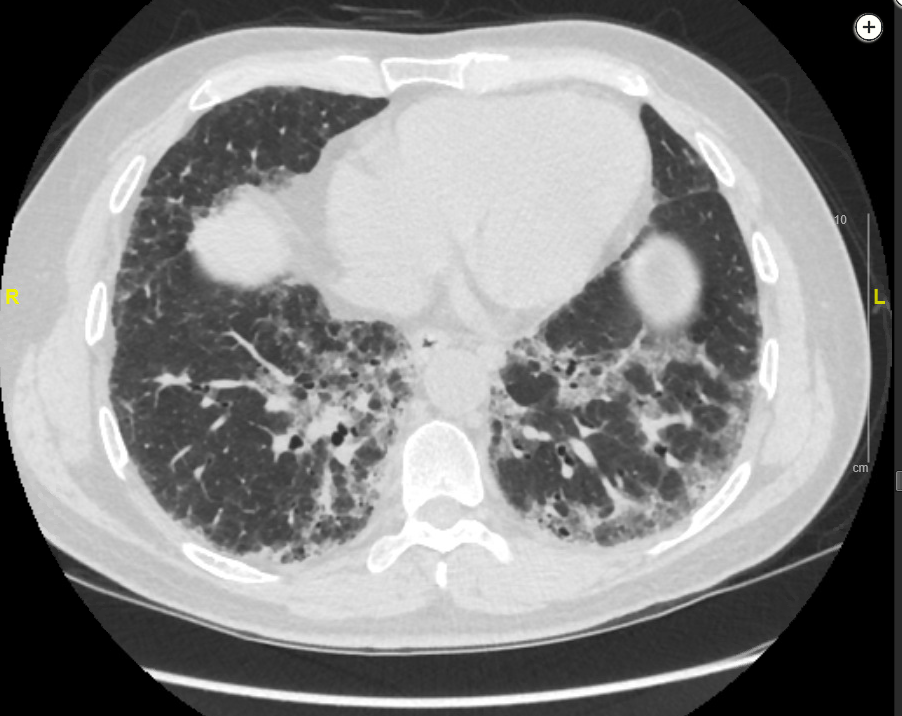
- CT scan: 2.peribronchovascular nodules and GGO
- biopsy: 2.hyperplastic lymphoid follicles with germinal centers, no plasma or granulomas
Follicular bronchiolitis is a type of constrictive bronchiolitis (constrictive bronchiolitis).
This patient has Sjögren syndrome with xerophthalmia, xerosis, and arthralgias, and he has developed a diffuse parenchymal lung disease with clinical, radiographic, and histological features most consistent with follicular bronchiolitis (FB).
FB is an uncommon bronchiolar disorder characterized by lymphoid hyperplasia of the bronchial-associated lymphoid tissue, distributed along bronchovascular bundles. FB can occur alone or, more typically, in association with an underlying immune, infectious, or inflammatory condition. Among the connective tissue disorders, Sjögren syndrome, rheumatoid arthritis, and systemic lupus erythematosus are most commonly associated with FB. The diagnosis and symptoms of an underlying connective tissue disease typically precede respiratory symptoms, as in this case. Associated immunodeficiency states can be congenital, like common variable immunodeficiency, or acquired, like HIV/AIDS. Infectious causes include Pneumocystis pneumonia, Legionella pneumonia, and active hepatitis. FB can also be a component of idiopathic interstitial pneumonias. Patients with FB vary in age, but the primary form tends to occur in middle-aged or older individuals (average is fifth decade). Pulmonary symptoms begin gradually, usually with cough and dyspnea. Fever and weight loss are also reported, as well as the symptoms common to the primary disease, such as arthralgias and arthritis in connective tissue diseases, and recurrent infections in immune disorders. Diagnosis is by surgical biopsy because transbronchial biopsy cannot provide an adequate tissue sample, and presentation is nonspecific. Histological evaluation allows for distinguishing FB from other closely related lymphoproliferative diseases and ruling out lymphoma, which occurs with an increased incidence in patients with Sjögren syndrome. Histologically, FB is characterized by multiple reactive lymphoid follicles with germinal centers distributed around bronchi and bronchioles. Airway wall infiltration can lead to narrowing of the bronchiolar lumen. Pulmonary function tests can show a restrictive, obstructive, or mixed pattern or may be normal in mild disease. A reduced diffusing capacity is commonly seen. Radiographic findings vary, though they typically include small bilateral centrilobular nodules and patchy ground-glass opacities. Other findings that can be seen include peribronchial nodules and a mosaic attenuation suggesting air trapping.
Patients diagnosed with FB should have serological testing for connective tissue diseases, as well as immune globulin levels, and HIV testing. Management usually starts with treating the underlying condition and may also include corticosteroids alone or in combination with another immunosuppressive drug, depending on clinical status and response to the selected regimen. Primary FB is treated with immunosuppressant drugs, with case reports also noting success with macrolide antibiotics. Outcome tends to be better when treatment is initiated early in the course of the disease. The patient presented here was placed on immunosuppressive agents but, despite treatment, progressed clinically and radiographically and ultimately went on to lung transplantation.
Nodular lymphoid hyperplasia presents with well-demarcated single or multiple masses, often subpleural (but may be peribronchial) on chest CT imaging. Histology shows interfollicular plasma cells in the nodular lymphoid tissue, sometimes with loose nonnecrotizing granulomas (choice B is incorrect).
Lymphoid interstitial pneumonia is also seen in patients with Sjögren syndrome and can overlap with FB because both are considered part of the spectrum of lymphoproliferative pulmonary diseases, though with distinct histopathology. Lymphoid interstitial pneumonia is characterized by a diffuse interstitial and alveolar septal infiltration of lymphocytes, plasma cells, and histiocytes. In addition, cysts are commonly seen on chest CT scans (choice C is incorrect).
IgG4-related disease can involve one or multiple organs and can present as mass lesions and/or organ enlargement. Lymphadenopathy is common. Patients can have symptoms similar to those of Sjögren syndrome, including sicca symptoms, arthralgias, and glandular enlargement, though anti-Ro and anti-La reactivity is not frequently found. Radiographically, IgG4-related disease can appear as solid nodular tumors, ground-glass opacities, alveolar interstitial changes, or thickened bronchovascular bundles. Histologically, a plasma lymphocytic infiltrate with abundant IgG4-positive plasma cells is seen (choice D is incorrect).1
Links to this note
-
ILD Interstitial Lung Disease or Diffuse Parenchymal Lung Disease
-
- lymphocytic: follicular bronchiolitis and LIP (lymphoid interstitial pneumonia LIP etiologies are typically autoimmune)